
WELCOME
This is the complete guide to the symptoms and latest treatment of trigeminal neuralgia for people in Singapore and Asia.
Trigeminal neuralgia is a nerve disorder that causes severe facial pain affecting half of the face.
Many people live with trigeminal pain throughout their lives, not knowing that there are many solutions ranging from reducing pain, improving quality of life to permanent cure that can free them from this painful affliction.
For questions or more information, please contact our clinic at (+65) 6592 6871.
Speak to a specialist for your facial pain today.

About Dr Nicolas Kon
Dr Nicolas Kon is a neurosurgeon in Singapore who specialises in trigeminal neuralgia and other neurological conditions. Dr Kon uses a patient-centered approach that has successfully helped many patients to deal with trigeminal neuralgia. With over 20 years of experience, he provides the full range of treatment for trigeminal neuralgia including medical therapy, non-invasive radiosurgery (Gamma Knife), radiofrequency ablation or injections, and minimally invasive microvascular decompression surgery.
Types of treatment for trigeminal neuralgia in Singapore offered by Dr Kon:




Who gets trigeminal neuralgia?
Prevalence
Trigeminal neuralgia can affect anyone. Worldwide, between 10 to 300 per 100,000 people have trigeminal neuralgia.
Demography
In Singapore, trigeminal neuralgia affects women more often than men. Although the peak age of onset is between ages 50 to 60, many young people are also affected.
Risk factors
The risk of getting trigeminal neuralgia appears higher in people with multiple sclerosis, hypertension, diabetes and family history of trigeminal neuralgia. But often, there are no risk factors identified.

Do you suffer from the excruciating pain of trigeminal neuralgia?
Trigeminal neuralgia is one of the most painful conditions known to affect people. Imagine feeling the pain of an electric shock on your cheek or the sensation of your skin burning. That’s what some trigeminal neuralgia patients face every day.
Trigeminal neuralgia is not life-threatening. But, when it is not properly managed, it means having to live with life-long, disabling pain.
For many people, it may take several months or even years to reach the correct treatment.

What are the symptoms of trigeminal neuralgia?
Type of pain
The pain is a severe, sudden electric shock or stabbing pain, usually on one side of the face. The right side is more commonly affected.
Areas of pain
Pain is felt in one half of the face, and specific to areas that are connected to the affected trigeminal nerve, especially around the eye, lower cheek and jaw. The nose and forehead are less affected.
Triggers
The pain is triggered by physical contact with the face or facial movement. In severe cases, even very mild stimulation of the face, such as brushing teeth, eating or talking, may provoke pain.
Frequency
Pain strikes intensely and repeatedly, lasting for a few seconds each time. Sometimes, a dull aching pain may follow and persist for minutes. Pain flare-ups can occur several times per day on a daily basis. Pain is completely gone between flare-ups.
Pattern of flare-ups
Over time, pain flare-ups become more intense and frequent. Pain-free periods (known as remission) become shorter and shorter until it becomes a constant pain. This usually happens when it is left untreated.
Atypical forms
Not everyone has the classic symptoms. Some experience a continuous pain with sensory deficits (such as numbness). These cases require more detailed investigations to rule out secondary causes of the pain.

How does trigeminal neuralgia compare to other pain?
Trigeminal neuralgia is also referred to as the “suicide disease” because it is one of the most painful conditions.
It is unrelenting. It is exhausting pain. Here is how trigeminal neuralgia compare with other types of pain.


Why do people get trigeminal neuralgia?
A blood vessel abnormally pressing on the trigeminal nerve is the most common culprit of the facial pain.
Demyelination
Demyelination refers to the wearing down the protective coating around the nerve (called "myelin sheath"), making it hypersensitive. The hypersensitive nerve ‘misfires’ at the slightest provocation akin to a "short circuitry". Over time, the myelin may try to heal itself, which can sometimes successfully buy some pain-free time.
Common causes
The most common cause of trigeminal neuralgia is a blood vessel, sometimes several, pressing on the trigeminal nerve. The pressure of the blood vessel on the nerve causes nerve injury and demyelination, which in turn manifests as the classic shooting, electrical pain.

Other possible causes are brain tumours pressing on the trigeminal nerve, or multiple sclerosis (which causes the myelin sheath to thin out).
How is trigeminal neuralgia diagnosed?
Pain characteristics
One of the criteria for the diagnosis of typical trigeminal neuralgia is the character of the pain itself. A comprehensive history of the patient, involving specifics of the nature of pain, affected facial areas and duration can be sufficient to raise the suspicion of a diagnosis. Careful evaluation by a specialist in trigeminal neuralgia is recommended.
MRI scan
A special magnetic resonance imaging (MRI) is performed to assess whether a nearby blood vessel is pressing down on the nerve. A diagnosis can be established if the patient has the typical symptoms, as well as a conflict between the nerve and its adjacent blood vessel on MRI.
Life pro tip:
Ask for a specialised MRI that increases the likelihood of finding the offending vessel, and do have your MRI reviewed by a specialist in trigeminal neuralgia.
When no conflict between the nerve and its adjacent blood vessel is seen on specialised MRI, the trigeminal neuralgia can be classified as idiopathic trigeminal neuralgia.


Trigeminal nerve and its pain zone
The fifth nerve
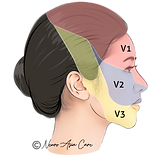
The trigeminal nerve is the fifth cranial nerve, and provides the face with the sense of touch, temperature and pain, as well as motor function to the muscles of mastication. The trigeminal nerve is divided into 3 branches which supplies to specific areas of the face.
Trigeminal nerve innervation zones
(spread of pain)
-
Ophthalmic nerve, V1 supplies to the eyes, forehead and scalp.
-
Maxillary nerve, V2 supplies to the cheeks, around the nose, upper lip, jaw, teeth and gums.
-
Mandibular nerve, V3 supplies to the bottom lip, jaw, teeth and gums.

V3 nerve compression is most common in Singapore.
In Singapore, V3 involvements is seen in 70% of patients with trigeminal neuralgia.
V3 nerve compression is more commonly seen among Asians, while Caucasian patients more frequently gets V2 compression. V3 (mandibular branch) supplies to the lower teeth. Hence, pain tend to start along the upper or lower teeth, making people think they have a dental or root canal problem.

This may explain why trigeminal neuralgia can be commonly mistaken as toothache or dental problem in Singapore. Some people seek repeated dental procedures in an attempt to treat the pain. When the pain persists, they realise that the pain is due to the nerve compression.

Comparison of the treatment options for trigeminal neuralgia
This is an overview of the complete treatment plan to manage trigeminal neuralgia. Remember that disease severity and patient requirements will change over time, and careful re-evaluation of your treatment plan is recommended. The key is to have a tailored treatment plan making very effective treatment of trigeminal neuralgia possible.
Types of treatment for trigeminal neuralgia in Singapore offered by Dr Kon:


In focus: This is a head-to-head comparison of the existing treatment for trigeminal neuralgia in Singapore, ranging from medical therapy, non-invasive radiosurgery (Gamma Knife), non-surgical radiofrequency ablation or injections, and minimally invasive microvascular decompression surgery.

Medication is the first-line treatment.

Medication is not a cure but works well in the early months or years to control the pain. Over time, they may lose effectiveness or cause intolerable side effects with increasing dose.
Anti-convulsants
Proper selection of the right medication is important. The most commonly prescribed drugs are anti-convulsant such as carbamazepine, (Tegretol). Other medications include gabapentin (Neurontin), pregabalin (Lyrica), phenytoin (Dilantin) and baclofen. They work by slowing down electrical impulse in the trigeminal nerve and reducing its ability to transmit pain.
Pre-testing
Before starting on carbamazepine, testing for HLA-B allele is recommended. The presence of the HLA-B allele increases the risk of developing toxic epidermal necrolysis or Stevens-Johnson syndrome. This is important to note as the allele is more commonly found in patients with Asian ancestry. In Singapore, the incidence of HLA-B allele is 12%.
When should you consider other treatment?
When medications prove to be ineffective or unsatisfactory, it is time to consider other treatment options.
The top 3 reasons in Singapore for people to change their treatment plan for trigeminal neuralgia are:
1. Your pain is not well controlled despite the best use of medication.
2. You experience side effects from medication (e.g., sleepiness, dizziness, forgetfulness, brain fog).
3. You do not wish to be on lifelong medication.
Microvascular decompression surgery is most effective.
Microvascular decompression has the best long term pain relief among all treatment options.
Life pro tip:
Ask your neurosurgeon about your individualized surgical risks and understand how they can be best managed.
Although microvascular decompression (MVD) is the most effective and only curative solution, many patients find the idea of surgery too scary. Compared to the past, contemporary surgery has been made much safer and more effective with the help of advanced tools, intraoperative neuromonitoring and minimally invasive approach.
Microvascular decompression (MVD)
If you are looking for a permanent cure, surgery is the ideal treatment as it treats the root of the problem. Contrary to what many believe, this is not brain surgery; it is a surgical procedure to the nerves at the base of the skull. The aim is to move the vein or artery away from nerve to relief the pressure on the nerve.
How is MVD surgery done?
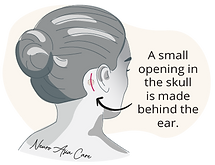

Minimally invasive microvascular decompression involves making a tiny opening in the skull behind the ear, locating the blood vessel and inserting a small Teflon sponge to separate the blood vessel and nerve. It is a very skilled procedure, but, in the right hands, the success rate is very good. It has almost immediate pain relief with high success rate of pain relief.
Gamma knife radiosurgery is non-invasive.
Gamma knife radiosurgery is painless, does not require opening of the skull and can be done as an outpatient procedure with minimal downtime.
Gamma Knife radiosurgery
For patients who do not want or are unsuitable for microvascular decompression, Gamma Knife radiosurgery is a good and popular treatment option. As its name suggests, it is incisionless and instead uses radiation to lesion or "cut into" the nerve root. Therefore, recovery time is minimal. One thing to note is that the effects of gamma knife is not instant. Maximum effect of pain relief is achieved at 3 months after the procedure is done.
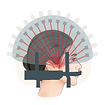
How is radiosurgery done?
A stereotactic frame is attached to the head to fix the head in position for maximum precision. The stereotactic radiosurgery machine focuses narrow beams of radiation onto one target point in the trigeminal root nerve to stop it from sending pain signals to the brain.


Radiofrequency ablation is minimally invasive.
Radiofrequency ablation is a minimally invasive surgical technique that is performed under sedation. It can be done as an outpatient procedure with minimal downtime.
Radiofrequency ablation
Radiofrequency ablation is the most common percutaneous rhizotomy procedure to treat trigeminal neuralgia. Glycerol rhizolysis and balloon compression are less popular. Radiofrequency ablation uses a needle to heat a part of the nerve. Pain reduction after radiofrequency ablation is immediate and the recovery time is minimal.
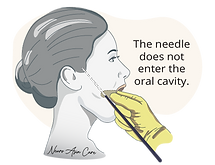
How is radiofrequency done?
A thin needle is inserted through the cheek into the trigeminal nerve root under X-ray fluoroscopic guidance. A low current of electricity stimulates the nerve to locate the areas of pain. Once the location is confirmed, a heated current is passed through the electrode to lesion a part the nerve.

Prognosis: Will the pain go away by itself?
No, the facial pain in trigeminal neuralgia, once established, is unlikely to go away on its own without treatment. But solutions are available that can help treat the pain.
Know your options. Speak to a neurosurgeon.
Seeing a neurosurgeon does not mean you are committing to surgery. Arm yourself with information with which to make your decision. If the time is right for you to consider surgery, see a neurosurgeon to assess your eligibility for this life-changing procedure that can free you from this painful affliction.
About Dr Nicolas Kon
Dr Nicolas Kon is a specialist neurosurgeon in Singapore who provides the full range of treatment for trigeminal neuralgia including medical therapy, non-invasive radiosurgery (Gamma Knife), radiofrequency ablation and injection, and minimally invasive microvascular decompression surgery.